Patrick S. Forscher en Twitter: “.@ThreeLittleMigs and I are polishing a health behavior for @PsySciAcc’s COVID project. We expect to reach thousands of participants all over the world. We want our survey to be useful to epidemiologists. Would any epidemiologists be willing to give us feedback? DM me if so!” / Twitter. (n.d.). Twitter. Retrieved April 17, 2020, from https://twitter.com/psforscher/status/1245923025221849091
8,968 Matching Annotations
- Apr 2020
-
twitter.com twitter.com
-
www.reddit.com www.reddit.com
-
r/BehSciResearch - Planned study: Inoculating against COVID-19 misinformation. (n.d.). Reddit. Retrieved April 17, 2020, from https://www.reddit.com/r/BehSciResearch/comments/futkvx/planned_study_inoculating_against_covid19/
-
-
twitter.com twitter.com
-
ReconfigBehSci en Twitter: “an interesting source of statistics, both on COVID-19 and other issues that help provide some context to numbers https://t.co/T0wBZIlCfR” / Twitter. (n.d.). Twitter. Retrieved April 17, 2020, from https://twitter.com/SciBeh/status/1246714565850734592
-
-
-
New CEPR publication: Covid Economics, Vetted and Real-Time Papers | Centre for Economic Policy Research. (n.d.). Retrieved April 17, 2020, from https://cepr.org/content/new-cepr-publication-covid-economics-vetted-and-real-time-papers
-
-
ec.europa.eu ec.europa.eu
-
EUvsVirus Hackathon to develop innovative solutions and overcome coronavirus-related challenges. (n.d.). [Text]. European Commission - European Commission. Retrieved April 17, 2020, from https://ec.europa.eu/info/news/euvsvirus-hackathon-develop-innovative-solutions-and-overcome-coronavirus-related-challenges-2020-apr-03_en
-
-
datascience.udd.cl datascience.udd.cl
-
Ferres, L., Schifanella, R., Perra, N., Vilella, S., Bravo, L., Paolotti, D., Ruffo, G., & Sacasa, M. (n.d.). Measuring Levels of Activity in a Changing City. 11.
-
-
www.combine.umd.edu www.combine.umd.edu
-
Network Epidemiology Online Workshop Series | COMBINE. (n.d.). Retrieved April 17, 2020, from http://www.combine.umd.edu/network-epidemiology/
-
-
www.buzzsprout.com www.buzzsprout.com
-
Old age and COVID-19—The Lancet Voice. (n.d.). Retrieved April 17, 2020, from https://www.buzzsprout.com/861868/3254377
-
-
www.livemint.com www.livemint.com
-
Opinion| Get rid of that tricky habit of touching your face. (2020, March 31). Livemint. https://www.livemint.com/opinion/columns/opinion-get-rid-of-that-tricky-habit-of-touching-your-face-11585599176439.html
-
-
www.cambridge.org www.cambridge.org
Tags
- Korea
- preparation
- community
- rule
- response
- communication
- risk
- lang:en
- control
- outbreak
- COVID-19
- is:article
- involvement
- diagnosis
Annotators
URL
-
-
covid19.gleamproject.org covid19.gleamproject.org
-
COVID-19 MODELING IN THE UNITED STATES. (n.d.). Retrieved April 17, 2020, from https://covid19.gleamproject.org/#
-
-
twitter.com twitter.com
-
Alex Holcombe en Twitter: “Finally journal editors are losing their lock on scholarship- COVID19 is speeding this up. @elife will ‘make the posting of preprints to bioRxiv or medRxiv the default for all eLife submissions’ @eLife ahead of the pack; the leaders are @Meta_Psy and other small journals. @SciBeh” / Twitter. (n.d.). Twitter. Retrieved April 17, 2020, from https://twitter.com/ceptional/status/1248353897195769857
-
-
twitter.com twitter.com
-
Carl Miller en Twitter: “We’re working hard at the moment to scale up our attempts to detect COVID-19 disinformation, online manipulation, attacks on public health officials and miracle cures. If you’ve come across this kind of stuff, I’d really appreciate hearing about it. DMs are open” / Twitter. (n.d.). Twitter. Retrieved April 17, 2020, from https://twitter.com/carljackmiller/status/1244569393440468997#annotations:9pvychrpeeqhh0_wtrrs1q
-
-
www.spiegel.de www.spiegel.de
-
SPIEGEL, D. (n.d.). Coronavirus: Jeder zweite Deutsche würde Handy-Tracking von Infizierten dulden - DER SPIEGEL - Netzwelt. Retrieved April 17, 2020, from https://www.spiegel.de/netzwelt/netzpolitik/coronavirus-jeder-zweite-deutsche-wuerde-handy-tracking-von-infizierten-dulden-a-1becd6c6-d8d2-4d50-ba4c-240e38ca802c
-
-
infotagion.com infotagion.com
-
Home. (n.d.). Infotagion. Retrieved April 17, 2020, from https://infotagion.com/
Tags
Annotators
URL
-
-
rocs.hu-berlin.de rocs.hu-berlin.de
-
Forecasts by Country. (n.d.). Retrieved April 17, 2020, from http://rocs.hu-berlin.de/corona/docs/forecast/results_by_country/
-
-
centerforinquiry.org centerforinquiry.org
-
Kreidler, M. (2020, March 25). CORONAVIRUS RESOURCE CENTER | Center for Inquiry. https://centerforinquiry.org/coronavirus/
-
-
www.equallyours.org.uk www.equallyours.org.uk
-
The equality and human rights impacts of Covid-19. (n.d.). Equally Ours. Retrieved April 17, 2020, from https://www.equallyours.org.uk/resources/the-equality-and-human-rights-impacts-of-covid-19/
-
-
www.ons.gov.uk www.ons.gov.uk
-
Deaths involving COVID-19, England and Wales—Office for National Statistics. (n.d.). Retrieved April 20, 2020, from https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19englandandwales/deathsoccurringinmarch2020
-
-
lists.ufl.edu lists.ufl.edu
-
LISTSERV 16.0—SOCNET Archives. (n.d.). Retrieved April 20, 2020, from https://lists.ufl.edu/cgi-bin/wa?A2=ind2004&L=SOCNET&P=9667
-
-
publons.com publons.com
-
Publons.com. (n.d.). Retrieved April 20, 2020, from https://publons.com/
-
-
scibeh.org scibeh.org
-
Hahn, U., Lagnado, D., Lewandowsky, S., & Chater, N. (2020). Crisis knowledge management: Reconfiguring the behavioural science community for rapid responding in the Covid-19 crisis [Preprint]. PsyArXiv. https://doi.org/10.31234/osf.io/hsxdk
-
-
doi.org doi.org
-
Jarvis, C. I., Zandvoort, K. V., Gimma, A., Prem, K., Group, C. C.-19 working, Klepac, P., Rubin, G. J., & Edmunds, W. J. (2020). Quantifying the impact of physical distance measures on the transmission of COVID-19 in the UK. MedRxiv, 2020.03.31.20049023. https://doi.org/10.1101/2020.03.31.20049023
-
-
www.psychologytoday.com www.psychologytoday.com
-
The Power of Altruism. (n.d.). Psychology Today. Retrieved April 20, 2020, from https://www.psychologytoday.com/blog/the-art-self-improvement/202004/the-power-altruism
-
-
www.axa-research.org www.axa-research.org
-
Exceptional Flash Call for Proposals: Mitigating risk in the wake of the... (n.d.). Retrieved April 20, 2020, from https://www.axa-research.org/fr/page/call-for-proposals-mitigating-risk-in-the-wake-of-the-covid-19-pandemic
-
-
www.sciencedirect.com www.sciencedirect.com
-
Webster, R. K., Brooks, S. K., Smith, L. E., Woodland, L., Wessely, S., & Rubin, G. J. (2020). How to improve adherence with quarantine: Rapid review of the evidence. Public Health. https://doi.org/10.1016/j.puhe.2020.03.007
-
-
solve.mit.edu solve.mit.edu
-
Solutions. (n.d.). MIT SOLVE. Retrieved April 20, 2020, from https://solve.mit.edu/challenges/health-security-pandemics
-
-
jamanetwork.com jamanetwork.com
-
Jewell, N. P., Lewnard, J. A., & Jewell, B. L. (2020). Predictive Mathematical Models of the COVID-19 Pandemic: Underlying Principles and Value of Projections. JAMA. https://doi.org/10.1001/jama.2020.6585
-
-
psyarxiv.com psyarxiv.com
-
Pennycook, G., McPhetres, J., Bago, B., & Rand, D. G. (2020, April 14). Predictors of attitudes and misperceptions about COVID-19 in Canada, the U.K., and the U.S.A. https://doi.org/10.31234/osf.io/zhjkp
-
-
www.natureindex.com www.natureindex.com
-
Rapid Registered Reports initiative aims to stop coronavirus researchers following false leads. (n.d.). Retrieved April 20, 2020, from https://www.natureindex.com/news-blog/rapid-registered-report-coronavirus-aims-to-stop-researchers-following-false-research-leads
-
-
onlinelibrary.wiley.com onlinelibrary.wiley.com
-
Niet, A. de, Waanders, B. L., & Walraven, I. (n.d.). The role of children in the transmission of mild SARS-CoV-2 infection. Acta Paediatrica, n/a(n/a). https://doi.org/10.1111/apa.15310
-
-
onlinelibrary.wiley.com onlinelibrary.wiley.com
-
Giangreco, G. (n.d.). Case fatality rate analysis of Italian COVID-19 outbreak. Journal of Medical Virology, n/a(n/a). https://doi.org/10.1002/jmv.25894
-
-
onlinelibrary.wiley.com onlinelibrary.wiley.com
-
Abdulla, A., Wang, B., Qian, F., Kee, T., Blasiak, A., Ong, Y. H., Hooi, L., Parekh, F., Soriano, R., Olinger, G. G., Keppo, J., Hardesty, C. L., Chow, E. K., Ho, D., & Ding, X. (n.d.). Project IDentif.AI: Harnessing Artificial Intelligence to Rapidly Optimize Combination Therapy Development for Infectious Disease Intervention. Advanced Therapeutics, n/a(n/a), 2000034. https://doi.org/10.1002/adtp.202000034
-
-
www.thelancet.com www.thelancet.com
-
Lancet, T. (2020). COVID-19 in the USA: A question of time. The Lancet, 395(10232), 1229. https://doi.org/10.1016/S0140-6736(20)30863-1
-
-
sciencebusiness.net sciencebusiness.net
-
Science|Business Database: Coronavirus Funding Opportunities. (n.d.). Science|Business. Retrieved April 20, 2020, from https://sciencebusiness.net/sciencebusiness-database-coronavirus-funding-opportunities
-
-
www.reddit.com www.reddit.com
-
r/BehSciResearch—Behavioural science research for guiding societies out of lockdown. (n.d.). Reddit. Retrieved April 20, 2020, from https://www.reddit.com/r/BehSciResearch/comments/g2bm09/behavioural_science_research_for_guiding/
-
-
trello.com trello.com
-
Collective Intelligence and COVID-19 | Trello. (n.d.). Retrieved April 20, 2020, from https://trello.com/b/STdgEhvX/collective-intelligence-and-covid-19
-
-
papers.ssrn.com papers.ssrn.com
-
Thunstrom, L., Newbold, S., Finnoff, D., Ashworth, M., & Shogren, J. F. (2020). The Benefits and Costs of Using Social Distancing to Flatten the Curve for COVID-19 (SSRN Scholarly Paper ID 3561934). Social Science Research Network. https://doi.org/10.2139/ssrn.3561934
-
-
www.thelancet.com www.thelancet.com
-
Meyer, J. P., Franco-Paredes, C., Parmar, P., Yasin, F., & Gartland, M. (2020). COVID-19 and the coming epidemic in US immigration detention centres. The Lancet Infectious Diseases, 0(0). https://doi.org/10.1016/S1473-3099(20)30295-4
-
-
sciencebusiness.net sciencebusiness.net
-
Imperial researchers develop lab-free COVID-19 test with results in less than an hour. (n.d.). Science|Business. Retrieved April 20, 2020, from https://sciencebusiness.net/network-updates/imperial-researchers-develop-lab-free-covid-19-test-results-less-hour
-
-
sciencebusiness.net sciencebusiness.net
-
Hackathons mobilise start-ups to combat COVID-19. (n.d.). Science|Business. Retrieved April 20, 2020, from https://sciencebusiness.net/news/hackathons-mobilise-start-ups-combat-covid-19
-
-
network.crowdhelix.com network.crowdhelix.com
-
COVID-19. (n.d.). The Crowdhelix Network. Retrieved April 20, 2020, from https://network.crowdhelix.com/covid-19
-
-
read.oecd-ilibrary.org read.oecd-ilibrary.org
-
Testing for COVID-19: A way to lift confinement restrictions—OECD. (n.d.). Retrieved April 21, 2020, from https://read.oecd-ilibrary.org/view/?ref=129_129658-l62d7lr66u&title=Testing-for-COVID-19-A-way-to-lift-confinement-restrictions
-
-
www.ukri.org www.ukri.org
-
COVID-19 therapy, vaccine, epidemiology and policy development research boosted by twenty-one new projects—UK Research and Innovation. (n.d.). Retrieved April 21, 2020, from https://www.ukri.org/news/covid-19-research-boosted-by-new-projects/
-
-
www.thelancet.com www.thelancet.com
-
Peto, J., Alwan, N. A., Godfrey, K. M., Burgess, R. A., Hunter, D. J., Riboli, E., Romer, P., Buchan, I., Colbourn, T., Costelloe, C., Smith, G. D., Elliott, P., Ezzati, M., Gilbert, R., Gilthorpe, M. S., Foy, R., Houlston, R., Inskip, H., Lawlor, D. A., … Yao, G. L. (2020). Universal weekly testing as the UK COVID-19 lockdown exit strategy. The Lancet, 0(0). https://doi.org/10.1016/S0140-6736(20)30936-3
-
-
www.thelancet.com www.thelancet.com
-
Ranscombe, P. (2020). Rural areas at risk during COVID-19 pandemic. The Lancet Infectious Diseases, 0(0). https://doi.org/10.1016/S1473-3099(20)30301-7
-
-
drive.google.com drive.google.com
-
Joint Statement.pdf. (n.d.). Google Docs. Retrieved April 21, 2020, from https://drive.google.com/file/d/1OQg2dxPu-x-RZzETlpV3lFa259Nrpk1J/view?usp=drive_open&usp=embed_facebook
-
-
twitter.com twitter.com
-
ReconfigBehSci en Twitter: “RT @paimadhu: I suspect most folks rushing to pre-prints with correlations between #Covid_19 & a host of variables (e.g. BCG, malaria endem…” / Twitter. (n.d.). Twitter. Retrieved April 21, 2020, from https://twitter.com/scibeh/status/1252311781382541312
-
-
-
Blog: Combatting COVID-19 through data: some considerations for privacy. (2020, April 17). ICO. https://ico.org.uk/about-the-ico/news-and-events/blog-combatting-covid-19-through-data-some-considerations-for-privacy/
-
-
www.abc.net.au www.abc.net.au
-
Deputy CMO doesn’t rule out forcing Australians to download contact tracing app. (2020, April 17). [Text]. ABC News. https://www.abc.net.au/news/2020-04-17/paul-kelly-coronavirus-tracing-app/12158854
-
-
-
Callaway, E. (2020). Should scientists infect healthy people with the coronavirus to test vaccines? Nature, 580(7801), 17–17. https://doi.org/10.1038/d41586-020-00927-3
-
-
metro.co.uk metro.co.uk
-
Social distancing “is a problematic term” that could damage our mental wellbeing. (2020, April 17). Metro. https://metro.co.uk/2020/04/17/swap-social-distancing-safe-relating-sake-wellbeing-12570403/
-
-
www.hcpc-uk.org www.hcpc-uk.org
-
Standards of conduct, performance and ethics |. (n.d.). Retrieved April 21, 2020, from https://www.hcpc-uk.org/standards/standards-of-conduct-performance-and-ethics/
-
-
twitter.com twitter.com
-
Daniel Summers, MD en Twitter: “‘Social distancing was unnecessary’ is the new ‘why should we vaccinate against diseases nobody gets any longer?’ https://t.co/kgB2Rwi4W8” / Twitter. (n.d.). Twitter. Retrieved April 21, 2020, from https://twitter.com/wfkars/status/1248220267115134978
-
-
www.thedailybeast.com www.thedailybeast.com
-
Summers, D. (2020, April 10). The Absurd Error Lockdown Skeptics and Anti-Vaxxers Both Make. The Daily Beast. https://www.thedailybeast.com/coronavirus-lockdown-skeptics-and-anti-vaxxers-make-same-absurd-error
-
-
twitter.com twitter.com
-
Leo Ferres en Twitter: “I’m trying to compile #COVID19 reports that use cellphone data around the world. I’ve done a few (see link below) https://t.co/LEr61QWERm Can you help me by leaving a message, or replying to this tweet or just email with a relevant document? Thanks!” / Twitter. (n.d.). Twitter. Retrieved April 21, 2020, from https://twitter.com/leoferres/status/1248644220249874432
-
-
sciencebusiness.net sciencebusiness.net
-
Interview: We should tackle COVID-19 head on, but now is not the time to cut basic research. (n.d.). Science|Business. Retrieved April 22, 2020, from https://sciencebusiness.net/news/interview-we-should-tackle-covid-19-head-now-not-time-cut-basic-research
-
-
-
Apr 21, P., & 2020. (2020, April 21). State Data and Policy Actions to Address Coronavirus. The Henry J. Kaiser Family Foundation. https://www.kff.org/health-costs/issue-brief/state-data-and-policy-actions-to-address-coronavirus/
-
-
-
Cheng, M. (n.d.). Uber is shifting from moving people to delivering essentials. Quartz. Retrieved April 22, 2020, from https://qz.com/1842402/uber-is-shifting-from-moving-people-to-delivering-essentials/
-
-
www.wifo.ac.at www.wifo.ac.at
-
WIFO - News Detail. (n.d.). Retrieved April 22, 2020, from https://www.wifo.ac.at/news/covid-19_oekonomische_effekte_auf_frauen
-
-
twitter.com twitter.com
-
Adam Kucharski en Twitter: “I’m seeing more and more suggestions that contact tracing and/or physical distancing isn’t needed and we could solve COVID-19 with widespread testing alone. E.g. just test everyone once a week/fortnight to get R<1. Sounds straightforward? Unfortunately not... 1/” / Twitter. (n.d.). Twitter. Retrieved April 22, 2020, from https://twitter.com/adamjkucharski/status/1252241817829019648
-
-
teaforteaching.com teaforteaching.com
-
Sure. So I do want to start by just reminding listeners that talking about trauma, learning about trauma, can bring up some feelings, which is a very normal reaction to that. So I just want to remind people, if you notice that, that it’s okay to take a rain check on listening and engaging in this conversation. I also do recommend that even if you feel okay to engage with a discussion about trauma that it’s recommended that you do so in small doses, especially during these very challenging times.
This is a lovely way to introduce this topic.
-
-
techcrunch.com techcrunch.com
-
Spontaneity is the big thing you'll miss
Forget the calendar invite. Just jump into a conversation. That’s the idea powering a fresh batch of social startups poised to take advantage of our cleared schedules amidst quarantine. But they could also change the way we work and socialize long after COVID-19 by bringing the free-flowing, ad-hoc communication of parties and open office plans online. While “Live” has become synonymous with performative streaming, these new apps instead spread the limelight across several users as well as the task, game, or discussion at hand.
-
-
www.askeladdencapital.com www.askeladdencapital.com
-
Based on all of these approaches, it seems like a reasonable lower bound is that cases are at least 10x underreported, likely more than 20x underreported (according to several researchers), and potentially as much as 100x underreported.It seems reasonable, then, to assume that it’s not 1 out of every 10 people with COVID-19 who will need hospitalization -but rather 1 out of every 100 -500.Similarly, rather than 1 -4%, it seems likely that true CFR for COVID-19 will be well under half a percent, and potentially well under 0.1%for most of the population.
-
-
virihealth.com virihealth.com
-
Long-Term Care Outbreaks
Long-Term Care Outbreaks. Can't find an official spot showing this information on the AB Health website.
-
-
www.atsjournals.org www.atsjournals.org
-
cute coronary syndrome (ACS)4/81(4.94%)
-
Malignant arrhythmia2/81(2.47%)
-
Patients presented with functional damage involving multiple vital organs, including respiratory failure (80 [94.1%]), shock (69 [81.2%]), ARDS (63 [74.1%]) arrhythmia (51 [60.0%]), acute myocardial injury (38 [44.7%]), acute liver injury (30 [35.3%]) and sepsis (28 [32.9%]) (Table 5)
-
Most patients had abnormal myocardial zymograms characterized by increased creatine kinase in 31 (36.5%) and increased lactate dehydrogenase in 70 (82.4%) patients.
-
The most common cause of death in 81 of the 85 patients was respiratory failure (38, 46.91%), followed by septic shock (16, 19.75%), multiple organ failure (13, 16.05%) and cardiac arrest (7, 8.64%).
-
-
onlinelibrary.wiley.com onlinelibrary.wiley.comTITLE2
-
In the epicenter of the current Italian epidemic, sudden cardiac death (SCD) likely occurred in many non-hospitalized patients with mild symptoms who were found dead home while in quarantine.
-
Even after hospital discharge, we should consider that myocardial injury might result in atrial or ventricular fibrosis, the substrate for subsequent cardiac arrhythmias
-
-
jamanetwork.com jamanetwork.com
-
However, a recent pathological study found scarce interstitial mononuclear inflammatory infiltrates in heart tissue without substantial myocardial damage in a patient with COVID-19,13 suggesting that COVID-19 might not directly impair the heart.
-
ompared with patients without cardiac injury, patients with cardiac injury presented with more severe acute illness, manifested by abnormal laboratory and radiographic findings, such as higher levels of C-reactive protein, NT-proBNP, and creatinine levels; more multiple mottling and ground-glass opacity; and a greater proportion requiring noninvasive or invasive ventilation.
-
Consistently, our study also found 19.7% of patients with cardiac injury and first demonstrated that cardiac injury was independently associated with an increased risk of mortality in patients with COVID-19.
-
After adjusting for age, preexisting cardiovascular diseases (hypertension, coronary heart disease, and chronic heart failure), cerebrovascular diseases, diabetes mellitus, chronic obstructive pulmonary disease, renal failure, cancer, ARDS, creatinine levels greater than 133 μmol/L, and NT-proBNP levels greater than 900 pg/mL, the multivariable adjusted Cox proportional hazard regression model showed a significantly higher risk of death in patients with cardiac injury than in those without cardiac injury, either during time from symptom onset (hazard ratio [HR], 4.26 [95% CI, 1.92-9.49]) or time from admission to study end point (HR, 3.41 [95% CI, 1.62-7.16]) (Table 3).
-
The mortality rate was higher among patients with vs without cardiac injury (42 [51.2%] vs 15 [4.5%]; P < .001) as shown in Table 2 and the Kaplan-Meier survival curves in Figure 2. The mortality rate increased in association with the magnitude of the reference value of hs-TNI
-
Patients with cardiac injury vs those without cardiac injury had shorter durations from symptom onset to follow-up (mean, 15.6 [range, 1-37] days vs 16.9 [range, 3-37] days; P = .001) and admission to follow-up (6.3 [range, 1-16] days vs 7.8 [range, 1-23] days; P = .039).
-
Of patients with cardiac injury, only 22 (26.8%) underwent examination of electrocardiogram (ECG) after admission, and 14 of 22 ECGs (63.6%) were performed during the periods of elevation of cardiac biomarkers. All 14 ECGs were abnormal, with findings compatible with myocardial ischemia, such T-wave depression and inversion, ST-segment depression, and Q waves. The ECG changes in 3 patients with representative cardiac injury are shown in eFigure 2 in the
-
In terms of radiologic findings, bilateral pneumonia (75 of 82 patients [91.5%] vs 236 of 334 patients [70.7%]) and multiple mottling and ground-glass opacity (53 [64.6%] vs 15 [4.5%]) were more prevalent in patients with than those without cardiac injury (both P < .001, Table 1).
-
The duration of hospitalization before testing was longer in patients with cardiac injury than those without cardiac injury (median [range] time, 3 [1-15] days vs 2 [1-8] days; P < .001).
-
The laboratory and radiologic findings are shown in Table 1. In the overall study population of 416 patients, median (IQR) levels of C-reactive protein (4.5 [1.4-8.5] mg/dL; to convert to milligrams per liter, multiply by 10) and procalcitonin (0.07 [0.04-0.15] ng/L) were elevated, while the median values of other laboratory indicators were within the normal range, such as counts of leukocytes, lymphocytes, platelets, erythrocytes; hemoglobin level; cardiac indicators
-
In the present study, we also found that markers of inflammatory response, such as C-reactive protein, procalcitonin, and leukocytes, were significantly increased among patients who suffered from cardiac injury. The activation or enhanced release of these inflammatory cytokines can lead to apoptosis or necrosis of myocardial cells.
-
Thus, because of the current limited evidence, the question of whether the SARS-CoV-2 virus can directly injure the heart requires further demonstration.
-
In terms of laboratory findings, patients with cardiac injury compared with patients without cardiac injury showed higher median leukocyte count (median [IQR], 9400 [6900-13 800] cells/μL vs 5500 [4200-7400] cells/μL), and levels of C-reactive protein (median [IQR], 10.2 [6.4-17.0] mg/dL vs 3.7 [1.0-7.3] mg/dL), procalcitonin (median [IQR], 0.27 [0.10-1.22] ng/mL vs 0.06 [0.03-0.10] ng/mL), CK-MB (median [IQR], 3.2 [1.8-6.2] ng/mL vs 0.9 [0.6-1.3] ng/mL), myohemoglobin (median [IQR], 128 [68-305] μg/L vs 39 [27-65] μg/L), hs-TNI (median [IQR], 0.19 [0.08-1.12] μg/L vs <0.006 [<0.006-0.009] μg/L), N-terminal pro-B-type natriuretic peptide (NT-proBNP) (median [IQR], 1689 [698-3327] pg/mL vs 139 [51-335] pg/mL),
-
Greater proportions of patients with cardiac injury required noninvasive mechanical ventilation (38 of 82 [46.3%] vs 13 of 334 [3.9%]; P < .001) or invasive mechanical ventilation (18 of 82 [22.0%] vs 14 of 334 [4.2%]; P < .001) than those without cardiac injury.
-
creatinine kinase–myocardial band (median [IQR], 3.2 [1.8-6.2] vs 0.9 [0.6-1.3] ng/mL)
-
N-terminal pro-B-type natriuretic peptide (median [IQR], 1689 [698-3327] vs 139 [51-335] pg/mL)
Tags
- covid-19 cardiac injury admission to follow-up duration
- covid-19 cardiac injury mechanical ventilation
- COVID-19 Pro-BNP
- COVID-19 cardiovascular cytokine storm
- covid-19 cardiac injury hospitalization time
- covid-19 cardiac injury mortality
- COVID-19 heart histological changes
- COVID-19 troponin
- covid-19 ECG
- covid-19 cardiac injury lung imaging findings
- COVID-19 cardiac injury
- covid-19 cardiac injury disease severity
- COVID-19 CK
Annotators
URL
-
-
jamanetwork.com jamanetwork.com
-
Moreover, hypoxemia caused by COVID-19 may bring about atrial fibrillation, which is the most common arrhythmia among elderly individuals, and atrial fibrillation could be refractory before the pulmonary function is improved.
-
-
Local file Local fileuntitled1
-
100 nM MLN-4760did not interfere with immunoprecipitation of ACE2 by S1-Ig,nor did this inhibitor interfere with S-protein-mediated infec-tion (Figure 4B and C)
hACE2 inhibitorm MLN-4760, does not interfere with immunoprecipitation of ACE2 by S1-Ig, nor did this inhibitor interfere with S-protein-mediated infection. So ACE2 inhibtor should not be a good way to interfere SARS infection
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
There were numerous differences in laboratory findings between patients admitted to the ICU and those not admitted to the ICU (Table 2), including higher white blood cell and neutrophil counts, as well as higher levels of D-dimer, creatine kinase, and creatine.
-
Thirty-six patients (26.1%) were transferred to the intensive care unit (ICU) because of complications, including acute respiratory distress syndrome (22 [61.1%]), arrhythmia (16 [44.4%]), and shock (11 [30.6%]).
-
Heart rate, respiratory rate, and mean arterial pressure did not differ between patients who received ICU care and patients who did not receive ICU care. These measures were recorded on day of hospital admission for all patients, then divided into those who were later admitted to the ICU or not.
-
Common complications among the 138 patients included shock (12 [8.7%]), ARDS (27 [19.6%]), arrhythmia (23 [16.7%]), and acute cardiac injury (10 [7.2%]). Patients who received care in the ICU were more likely to have one of these complications than non-ICU patients.
-
-
jamanetwork.com jamanetwork.com
-
The mortality during hospitalization was 7.62% (8 of 105) for patients without underlying CVD and normal TnT levels,
-
for those without underlying CVD but elevated TnT levels, and 69.44% (25 of 36) for those with underlying CVD and elevated TnTs.
-
Plasma TnT levels demonstrated a high and significantly positive linear correlation with plasma high-sensitivity C-reactive protein levels (β = 0.530, P < .001) and N-terminal pro–brain natriuretic peptide (NT-proBNP) levels (β = 0.613, P < .001). Plasma TnT and NT-proBNP levels during hospitalization (median [interquartile range (IQR)], 0.307 [0.094-0.600]; 1902.00 [728.35-8100.00]) and impending death (median [IQR], 0.141 [0.058-0.860]; 5375 [1179.50-25695.25]) increased significantly compared with admission values (median [IQR], 0.0355 [0.015-0.102]; 796.90 [401.93-1742.25]) in patients who died (P = .001; P < .001), while no significant dynamic changes of TnT (median [IQR], 0.010 [0.007-0.019]; 0.013 [0.007-0.022]; 0.011 [0.007-0.016]) and NT-proBNP (median [IQR], 352.20 [174.70-636.70]; 433.80 [155.80-1272.60]; 145.40 [63.4-526.50]) was observed in survivors
-
During hospitalization, patients with elevated TnT levels had more frequent malignant arrhythmias, and the use of glucocorticoid therapy (37 [71.2%] vs 69 [51.1%]) and mechanical ventilation (41 [59.6%] vs 14 [10.4%]) were higher compared with patients with normal TnT levels.
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.govmain.pdf1
-
that the levels of the last test of neutrophils (14/16, 87.5%), PCT (11/11, 100%), CRP (11/13, 84.6%), cTnI (7/9, 77.8%),
-
-
www.onlinejacc.org www.onlinejacc.org
-
In severe cases, COVID-19 may present as pneumonia, the acute respiratory distress syndrome (ARDS), with or without both distributive and cardiogenic shock, to which elderly populations with preexisting medical comorbidities are the most vulnerable
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
No study has described the incidence of ST-segment elevation myocardial infarction in COVID-19, but it appears to be low. Similarly, the incidence of left ventricular systolic dysfunction, acute left ventricular failure and cardiogenic shock have also not been described.
-
However, an elevation of high-sensitivity cardiac troponin I (cTnI) above 99th percentile upper reference limit is the most commonly used definition
-
-
onlinelibrary.wiley.com onlinelibrary.wiley.com
-
We describe the first case of acute cardiac injury directly linked to myocardial localization of severe acute respiratory syndrome coronavirus (SARS‐CoV‐2) in a 69‐year‐old patient with flu‐like symptoms rapidly degenerating into respiratory distress, hypotension, and cardiogenic shock.
-
An intra‐aortic balloon pump (IABP) was placed on top of adrenaline (0.07 μg/kg/min), and noradrenaline (0.1 μg/kg/min) was added for worsening hypotension (systolic blood pressure: 80/67/60 mmHg).
-
The first echocardiography showed a dilated left ventricle [left ventricular (LV) end‐diastolic diameter 56 mm], severe and diffuse LV hypokinesia (LV ejection fraction 34%). Three hours later, LV ejection fraction dropped to 25% and estimated cardiac index was 1.4 L/min/m2. Coronary angiography findings were unremarkable.
-
Vice versa, we did not observe viral particles in cardiac myocytes and, therefore, we cannot infer on viral cardiotropism. Cardiac myocytes showed non‐specific damage that was mainly characterized by focal myofibrillar lysis. In addition, we did not observe cytopathic endothelia and small intramural vessel inflammation or thrombosis. Other cases are needed to confirm this observation.
-
Cardiac myocytes showed non‐specific features consisting of focal myofibrillar lysis, and lipid droplets. We did not observe viral particles in myocytes and endothelia. Small intramural vessels were free from vasculitis and thrombosis. EMB did not show significant myocyte hypertrophy or nuclear changes; interstitial fibrosis was minimal, focal, and mainly perivascular
-
The pathologic study showed low‐grade interstitial and endocardial inflammation (Figure 1A and 1B). Large (>20 μm), vacuolated, CD68‐positive macrophages were seen with immune‐light microscopy (Figure 1C and 1D); they were ultrastructurally characterized by cytopathy, with membrane damage and cytoplasmic vacuoles (Figure 1E). The ultrastructural study demonstrated single or small groups of viral particles with the morphology (dense round viral envelope and electron‐dense spike‐like structures on their surface) and size (variable between 70 and 120 nm) of coronaviruses (Figure 2). COVID‐19 infected Vero cells were used as control. The viral particles were observed in cytopathic, structurally damaged interstitial cells that demonstrated loss of the cytoplasmic membrane integrity (Figure 3)
-
-
www.thelancet.com www.thelancet.com
-
By the end of Jan 25, 31 (31%) patients had been discharged and 11 (11%) patients had died; all other patients were still in hospital (table 1). The first two deaths were a 61-year-old man (patient 1) and a 69-year-old man (patient 2). They had no previous chronic underlying disease but had a long history of smoking.
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
The clinical effects of pneumonia have been linked to increased risk of cardiovascular disease up to 10-year follow-up16 and it is likely that cases infected via respiratory virus outbreaks will experience similar adverse outcomes. Therapeutic use of corticosteroids further augments the possibility of adverse cardiovascular events. However, long-term follow-up data concerning the survivors of respiratory virus epidemics are scarce. Lipid metabolism remained disrupted 12 years after clinical recovery in a metabolomic study amongst 25 SARS survivors,17 whereas cardiac abnormalities observed during hospitalisation in eight patients with H7N9 influenza returned to normal at 1-year follow-up.
-
-
academic.oup.com academic.oup.com
-
The final diagnosis was acute virus-negative lymphocytic myocarditis associated with SARS-CoV-2 respiratory infection
-
EMB (Panel E, day 7) documented diffuse T-lymphocytic inflammatory infiltrates (CD3+ >7/mm2) with huge interstitial oedema and limited foci of necrosis. No replacement fibrosis was detected, suggesting an acute inflammatory process. Molecular analysis showed absence of the SARS-CoV-2 genome within the myocardium. No contraction band necrosis or TTS-associated microvascular abnormalities were observed.
-
CMR (day 7) showed a recovery of systolic function (from 52% by CTA to 64% by CMR), although with persistence of a mild hypokinesia at basal and mid left ventricular segments; at the same sites, diffuse myocardial oedema, determining wall pseudo-hypertrophy, was observed on short T1 inversion recovery (STIR) sequences (Panel D) and confirmed by T1 and T2 mapping (average native T1 = 1188 ms, normal value <1045; average T2 = 61 ms, normal value <50). Late gadolinium enhancement sequences demonstrated absence of detectable myocardial scar/necrotic foci.
-
Although the first clinical suspicion was myocarditis, coronary computed tomography angiography (CTA) was acquired to rule out coronary artery disease (CAD). Baseline chest scan (Panel B) confirmed bilateral patchy ground-glass opacities; CTA showed no aortic dissection, pulmonary embolism, or epicardial CAD (Panel C). Dynamic 3D volume-rendering reconstruction demonstrated a clear hypokinesia of the left ventricle mid and basal segments, with normal apical contraction, suggesting a reverse Tako-Tsubo syndrome (TTS) pattern
-
ECG (Panel A) showed low atrial ectopic rhythm, mild ST-segment elevation in leads V1–V2 and aVR, reciprocal ST depression in V4–V6, and QTc 452 ms with diffuse U-waves. The high-sensitivity troponin T curve was 135–107–106 ng/L (normal value <14), NT-proBNP 512 pg/mL (normal value <153), and C-reactive protein 18 mg/L (normal value <6). Transthoracic echocardiogram showed mild left ventricular systolic dysfunction (LVEF 43%) with inferolateral wall hypokynesis; neither ventricle was dilated and there was no pericardial effusion.
-
-
www.ahajournals.org www.ahajournals.org
-
Itis likely that cardiac troponin measurements wererequested in those who were more unwell or where there wasreasonable suspicion of myocardial ischemia or myocardial dysfunction. Only systematic testing of both symptomatic and asymptomatic patients infected with SARS-CoV-2 will provide an accurate estimate of the prevalence of myocardial injuryin this condition.
-
In a cohort of 191 patients with confirmed COVID-19 based on SARS-CoV-2 RNA detection, the univariable odds ratio for death when hs-cTnI concentrations were above the 99thpercentile upper reference limit was 80.1 (95% confidence interval [CI]10.3 to 620.4, P<0.0001).[4]This was higher than the odds ratios observed for all other biomarkerstested,including D-Dimer and lymphocyte count.
-
-
jamanetwork.com jamanetwork.com
-
While the spectrum of clinical manifestation is highly related to the inflammation process of the respiratory tract, this case provides evidence of cardiac involvement as a possible late phenomenon of the viral respiratory infection. This process can be subclinical with few interstitial inflammatory cells, as reported by an autopsy study,10 or can present with overt manifestations even without respiratory symptoms, as in the present case.
-
A 12-lead electrocardiogram (ECG) showed low voltage in the limb leads, minimal diffuse ST-segment elevation (more prominent in the inferior and lateral leads), and an ST-segment depression with T-wave inversion in lead V1 and aVR
-
Chest radiography was repeated on day 4 and showed no thoracic abnormalities. Transthoracic echocardiography, performed on day 6, revealed a significant reduction of LV wall thickness (interventricular septum, 11 mm; posterior wall, 10 mm), an improvement of LVEF to 44%, and a slight decrease of pericardial effusion (maximum, 8-9 mm). At the time of submission, the patient was hospitalized with progressive clinical and hemodynamic improvement.
-
During the first days of her hospitalization, the patient remained hypotensive (systolic blood pressure less than 90 mm Hg) and required inotropic support (dobutamine) in the first 48 hours, during which there was a further increase in levels of NT-proBNP (8465 pg/mL), high-sensitivity troponin T (0.59 ng/mL), and creatine kinase–MB (39.9 ng/mL), with a progressive stabilization and reduction during the following days (Table). Blood pressure progressively stabilized, although systolic pressure remained less than 100 mm Hg, and dobutamine treatment was weaned on day 4.
-
Transthoracic echocardiography revealed normal left ventricular (LV) dimensions with an increased wall thickness (interventricular septum, 14 mm, posterior wall, 14 mm) and a diffuse echo-bright appearance of the myocardium. There was diffuse hypokinesis, with an estimated LV ejection fraction (LVEF) of 40%. There was no evidence of heart valve disease. Left ventricular diastolic function was mildly impaired with mitral inflow patterns, with an E/A ratio of 0.7 and an average E/e′ ratio of 12. There was a circumferential pericardial effusion that was most notable around the right cardiac chambers (maximum, 11 mm) without signs of tamponade. Cardiac magnetic resonance imaging (MRI) confirmed the increased wall thickness with diffuse biventricular hypokinesis, especially in the apical segments, and severe LV dysfunction (LVEF of 35%) (Video 1 and Video 2). Short tau inversion recovery and T2-mapping sequences showed marked biventricular myocardial interstitial edema. Phase-sensitive inversion recovery sequences showed diffuse late gadolinium enhancement extended to the entire biventricular wall (Figure 2). The myocardial edema and pattern of late gadolinium enhancement fulfilled all the Lake Louise criteria for the diagnosis of acute myocarditis.6 The circumferential pericardial effusion was confirmed, especially around the right cardiac chambers (maximum, 12 mm).
-
Cardiac magnetic resonance imaging showed increased wall thickness with diffuse biventricular hypokinesis, especially in the apical segments, and severe left ventricular dysfunction (left ventricular ejection fraction of 35%). Short tau inversion recovery and T2-mapping sequences showed marked biventricular myocardial interstitial edema, and there was also diffuse late gadolinium enhancement involving the entire biventricular wall. There was a circumferential pericardial effusion that was most notable around the right cardiac chambers. These findings were all consistent with acute myopericarditis.
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
In addition, repeated floods of catecholamines due to anxiety and the side effects of medication can also lead to myocardial damage.
-
Third, Huang’s study noted that high concentration of IL-1β, IFN-γ, IP-10 and MCP-1 could be detected in patients infected with 2019-nCoV, which might lead to activated T-helper-1 (Th1) cell responses [4]. Furthermore, they also found that ICU patients had much higher concentrations of inflammatory factors than those non-ICU patients, suggesting that the cytokine storm was associated with disease severity
-
Second, hypoxaemia may be also an important reason of cardiac injury. In Huang’s study, 32% COVID-19 patients had various degree of hypoxaemia and need required high-flow nasal cannula or higher-level oxygen support. In Chen’s study, up to 76% of patients require oxygen therapy. Due to severe 2019-nCoV infection, the pneumonia may cause significant gas exchange obstruction, leading to hypoxaemia, which significantly reduces the energy supply by cell metabolism, and increases anaerobic fermentation, causing intracellular acidosis and oxygen free radicals to destroy the phospholipid layer of cell membrane. Meanwhile, hypoxia-induced influx of calcium ions also leads to injury and apoptosis of cardiomyocytes.
-
The data again showed a significant higher incidence of acute cardiac injury in ICU/severe patients compared to the non-ICU/severe patients [RR = 13.48, 95% CI (3.60, 50.47), Z = 3.86, P = 0.0001]
-
Another two studies only gave the data of creatine kinase, if it can be seen as a biomarker of cardiac injury, the proportion might be 11.5% (95% CI 7.8–15.2%).
-
Two studies that gave clear data were statistically analyzed, and the data showed that 8.0% (95% CI 4.1–12.0%) patients might be suffered from an acute cardiac injury.
-
-
jamanetwork.com jamanetwork.com
-
It is reasonable to expect that severe and critical cases have more severe effects on the cardiovascular system owing to more robust inflammatory response. At this early stage, our knowledge is mainly based on available numerators data, and the exact population-level denominators are not known. Also, it is likely that the asymptomatic and mildly symptomatic cases are missing from most reports, which further skews our understanding of the disease.
-
-
www.thelancet.com www.thelancet.com
-
There were no obvious histological changes seen in heart tissue, suggesting that SARS-CoV-2 infection might not directly impair the heart
-
There were a few interstitial mononuclear inflammatory infiltrates, but no other substantial damage in the heart tissue
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
Based on the analysis of the clinical data, we confirmed that some patients died of fulminant myocarditis. In this study, we first reported that the infection of SARS-CoV-2 may cause fulminant myocarditis.
-
Among the 68 fatal cases, 36 patients (53%) died of respiratory failure, five patients (7%) with myocardial damage died of circulatory failure, 22 patients (33%) died of both, and five remaining died of an unknown cause
-
-
www.thelancet.com www.thelancet.com
-
There were a few interstitial mononuclear inflammatory infiltrates, but no other substantial damage in the heart tissue
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
Among survivors, secondary infection, acute kidney injury, and acute cardiac injury were observed in one patient each, occurring 9 days (acute kidney injury), 14 days (secondary infection), and 21 days (acute cardiac injury) after illness onset.
-
Creatine kinase, U/L≤1851 (ref)......>1852·56 (1·03–6·36)0·043....High-sensitivity cardiac troponin I, pg/mL≤281 (ref)......>2880·07 (10·34–620·36)<0·0001....
-
In this study, increased high-sensitivity cardiac troponin I during hospitalisation was found in more than half of those who died.
-
Heart failure44 (23%)28 (52%)16 (12%)<0·0001Septic shock38 (20%)38 (70%)0<0·0001Coagulopathy37 (19%)27 (50%)10 (7%)<0·0001Acute cardiac injury33 (17%)32 (59%)1 (1%)<0·0001Acute kidney injury28 (15%)27 (50%)1 (1%)<0·0001
-
-
onlinelibrary.wiley.com onlinelibrary.wiley.com
-
COVID‐19 prognosis is related to age and sex. The expression of ACE2 decreases with increasing age. ACE2 expression is higher in young people than in elderly individuals and higher in females than in males.11, 12 This pattern does not match the characteristic of severely ill COVID‐19 patients being mostly elderly males. We believe that whether the level of ACE2 expression is high or low is not a key factor affecting the prognosis of patients with COVID‐19. The relationship between sex and prognosis requires additional data to verify.
some believe that ACe2 level of expression does not correlate covid-19 prognosis
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
Duration from onset of symptoms to radiological confirmation of pneumonia, days5 (3–9)5 (3–7)Duration from onset of symptoms to ICU admission, days9 (6–12)11 (7–14)Heart rate, beats per min89 (20)89 (15)Systolic blood pressure, mm Hg133 (20)140 (21)
-
Cardiac injury3 (15%)9 (28%)12 (23%)
-
By Jan 26, 2020, 710 patients had been admitted to Wuhan Jin Yin-tan hospital with confirmed SARS-CoV-2 pneumonia, of whom 658 (93%) were considered ineligible, including three patients who had cardiac arrest immediately after admission.
-
-
www.ncbi.nlm.nih.gov www.ncbi.nlm.nih.gov
-
A raised troponin (hypersensitive-troponin I (hs-cTnI)) was detected in five patients, possibly suggestive of virus-associated myocardial injury.
-
-
www.nature.com www.nature.com
-
The mechanism of acute myocardial injury caused by SARS-CoV-2 infection might be related to ACE2. ACE2 is widely expressed not only in the lungs but also in the cardiovascular system and, therefore, ACE2-related signalling pathways might also have a role in heart injury.
-
Other proposed mechanisms of myocardial injury include a cytokine storm triggered by an imbalanced response by type 1 and type 2 T helper cells
-
Among the people who died from COVID-19 reported by the NHC, 11.8% of patients without underlying CVD had substantial heart damage, with elevated levels of cTnI or cardiac arrest during hospitalization.
-
and respiratory dysfunction and hypoxaemia caused by COVID-19, resulting in damage to myocardial cells.
-
some of the patients first went to see a doctor because of cardiovascular symptoms. The patients presented with heart palpitations and chest tightness rather than with respiratory symptoms, such as fever and cough, but were later diagnosed with COVID-19.
-
-
www.unaids.org www.unaids.org
-
www.unaids.org www.unaids.org
-
agenciaocote.com agenciaocote.com
-
-
www.weforum.org www.weforum.org
-
being open with people and securing their trust is vitally important. “The key to our success has been absolute transparency with the public – sharing every detail of how this virus is evolving, how it is spreading and what the government is doing about it, warts and all.”
-
there was no lockdown in South Korea. It did, however, close its schools. There have been postponed attempts at reopening them, but reopen they must, according to Foreign Minister Kang.
-
“Testing is absolutely critical with a fast-travelling virus like this,” says Kang. “We have tested over 350,000 cases so far – some patients are tested many times before they are released, so we can say they are fully cured. Altogether, we’re talking about one out of 145 or one out of 150 people having been tested so far.”
-
“We took an all-government approach. The Prime Minister created a task force of all government ministries and, crucially, all regional and city governments, too – we are a very devolved democracy.” This joined-up strategy, involving the different regional authorities around the country soon paid off. “When one region ran out of hospital beds we asked other provinces to open up beds in their hospitals. When it ran out of doctors we asked doctors in other regions to help,” she continues.
-
-
old.cognitive-edge.com old.cognitive-edge.com
-
where the dragon is an enchanted prince, where the handsome prince is a nasty thief, and where the thief saves the day
Keep our eyes open to discovery. Inquiry approaches help set the conditions for this kind of openness.
-
We find Alper et al.'s (2000) concept of "conflict efficacy" useful: it says that conflict should be measured not by its nature or origin, but by its contribution to the perception among group members that conflicts can and are dealt with productively.
How do we establish hyper local conflict efficacy while engaged in participatory action research?
-
Ravn (1998) poses the interesting possibility that Thomas' definition of conflict includes in it both productive and unproductive conflict, because productive conflict stops before it gets to the third phase of non-acceptance, instead using the energy of conflict as a positive force.
Productive conflict surfaces pain points and theories of causality from different stakeholder perspective, but does so without getting the point of non-acceptance.
-
Skule (1999) describes how an inter-organisational group of workers from five food-and-drink companies were taken through a training program that included "practice in other companies". Says Skule, "Most of the skilled operators described [the experience] in terms like "see things differently", “opened my eyes”, “think more about what I am doing”, “more alert” and “think more about the consequences”. These new perspectives or ways of seeing in turn made operators attend to features in their work situation in a new way. From a former habitual way of working according to minimum standards, many skilled operators developed a more reflectively skilled way of performing their job, within the limits of existing job structures and routines." We believe this kind of benefit may not be as often used as is possible.
Having teachers participate in laboratory classroom residencies has had this impact, but communicating the importance to experts is a challenge, and the tyranny of experts is to deny the importance of practitioners gaining insight or seeing new possibilities.
-
The strength of unwritten rules is that they are habitual within the group and thus both adaptive and resilient. Good management practice creates habits rather than rules. Coming
I like creating and testing protocols with peers to develop productive, generative routines. We set aside protocols when the routine suggests new possibilities, and develop new protocols when the routine fails to be productive or generative.
-
Inter-organisational networks help organisations sustain productive rule networks
The development of rule networks is critical right now in education. We've needed to establish rule networks to help practitioners understand the unreliability of standardized test data and develop agentive identities that aren't bound to those data sets. Now, in the absence of standardized tests in the US (they've been cancelled this year), charged with helping students learn while schools are closed, we need to establish rule networks that foster empathy and responsiveness to the needs of the community. At the same time we need rule networks that allow for experimentation and discovery.
-
In rejecting managerialism, we can equally discover the tyranny of the expert, as in Orwell’s nightmare the animals look through the window of the farm to see the pigs dressed as men.
The tyranny of the expert seems in part to deny the validity of the experience of the practitioners.
-
What inter-organisational networks provide is the opportunity for employees to discover this paradox for themselves through learning about the experiences of people at other organisations, and in the process to change how they manage their own constellation of identities in relation to their organisation.
Practitioners gain valuable perspective when they are engaged with a community of practice. Inter-organizational networks seem vital to the development of meaningful participatory action research.
-
The most effective systems leave a sufficient level of inefficiency in order that they can be resilient in changing contexts.
This reminds me of the inefficiency of educational technology staff and professional learning in schools. Trainers and coaches can be seen as inefficient because change is slow and implementation of digital tools is uneven and seemingly detached from performance metrics. Still, having people who are knowledgeable and capable of providing job-embedded coaching and support is vital at a time like this, when schools are called upon to be resilient.
-
Idealistic approaches tend to privilege expert knowledge, analysis and interpretation. Naturalistic approaches emphasise the inherent un-knowability of current and future complexities, and thus they de-privilege expert interpretation in favor of enabling emergent meaning at the ground level.
This concept was discussed in yesterday's webinar. As we look to the scientific community, we instinctively expect them to be able to present a complete picture of COVID-19, and we expect problem solving to be top down and efficient.
-
-
www.washingtonpost.com www.washingtonpost.com
-
In China, where the mortality rate for men was almost twice as high as that for women, nearly half of men over 15 smoke, compared with just 2 percent of women.
Huge difference! Wow!
-
-
www.ft.com www.ft.com
-
we face two particularly important choices. The first is between totalitarian surveillance and citizen empowerment. The second is between nationalist isolation and global solidarity.
Both of these feel like false choices.
-
Entire countries serve as guinea-pigs in large-scale social experiments. What happens when everybody works from home and communicates only at a distance? What happens when entire schools and universities go online? In normal times, governments, businesses and educational boards would never agree to conduct such experiments. But these aren’t normal times.
These questions suggest the importance of hyperlocal communities of practice that are engaged in safe-to-fail experiments under these larger areas of shift and potential inquiry.
-
Instead of every country trying to do it locally and hoarding whatever equipment it can get, a co-ordinated global effort could greatly accelerate production and make sure life-saving equipment is distributed more fairly.
The governor of New York just proposed sharing ventilators nationally to help states meet their needs. He's also redistributing ventilators around the state.
-
When people are told the scientific facts, and when people trust public authorities to tell them these facts, citizens can do the right thing even without a Big Brother watching over their shoulders. A self-motivated and well-informed population is usually far more powerful and effective than a policed, ignorant population.
These conditions seem like a very high bar nationally but perhaps not locally or hyperlocally.
-
But temporary measures have a nasty habit of outlasting emergencies, especially as there is always a new emergency lurking on the horizon.
In education we've taken temporary measures related to technology use and access. Students without devices are provided devices by schools, and also provided free access to the Internet.
Teachers, many of whom have had little training, are suddenly charged with teaching online.
-
One of the problems we face in working out where we stand on surveillance is that none of us know exactly how we are being surveilled, and what the coming years might bring. Surveillance technology is developing at breakneck speed, and what seemed science-fiction 10 years ago is today old news.
This is particularly true because of the use of AI. "Dressing for the Surveillance Age," by John Seabrook explains how researchers have to interact with the surveillance systems in order to develop ways to trick them.
Goldstein’s research is ultimately aimed at understanding these vulnerabilities, and making A.I. systems more secure. He explained that he and his student Zuxuan Wu were able to create a pattern that confuses the network using the same trial-and-error methods employed in training the neural network itself. “If you just try random patterns, you will never find an adversarial example,” he said. “But if you have access to the system you can find a pattern to exploit it.” To make the sweatshirt, they started with a pattern that looked like random static.
https://www.newyorker.com/magazine/2020/03/16/dressing-for-the-surveillance-age
-
But with coronavirus, the focus of interest shifts. Now the government wants to know the temperature of your finger and the blood-pressure under its skin.
In the development of a medical defense against a pandemic, it is vital that we remember that the horrible kinds of triage decisions hospitals are making right now would be less likely if these kinds of digitally mediated emergency measures were developed and ready to deploy.
-
This kind of technology is not limited to east Asia.
This kind of technology is ubiquitous here in the US, too. Our infrastructure is just more commercial by nature. This NY Times piece details just how trackable we all are using data gathered from mobile apps. https://www.nytimes.com/2019/12/19/opinion/tracking-phone-data.html
-
-
-
Welcome to ACUE’s Online Teaching Toolkit
Tags
Annotators
URL
-
-
jamanetwork.com jamanetwork.com
-
link-springer-com.ezproxy.javeriana.edu.co link-springer-com.ezproxy.javeriana.edu.co
-
www.ciwati.it www.ciwati.it
-
Passano le stagioni, ma solo quelle di Netflix.
eh già
-
- Mar 2020
-
link-springer-com.ezproxy.javeriana.edu.co link-springer-com.ezproxy.javeriana.edu.co
-
https://doi.org/10.1097/CCM.0000000000004363 DOI:10.1007/s00134‑020‑06022‑5
-
-
-
wearing simple face masks which exert a barrier function that blocks those big projectile droplets that land in the nose or throat may substantially reduce the production rate R, to an extent that may be comparable to social distancing and washing hands.
Most important message of the article
-
Make sure to discard or launder after use without touching the outward surface
What to do with a mask after usage
-
CDC suggests use of scarf by health care providers as last resort when no face masks are available
Use of scarf
-
avoiding large droplets, which cannot enter the lung anyway but land in the upper respiratory tracts, could be the most effective means to prevent infection. Therefore, surgical masks, perhaps even your ski-mask, bandanas or scarf
Wear a mask!
-
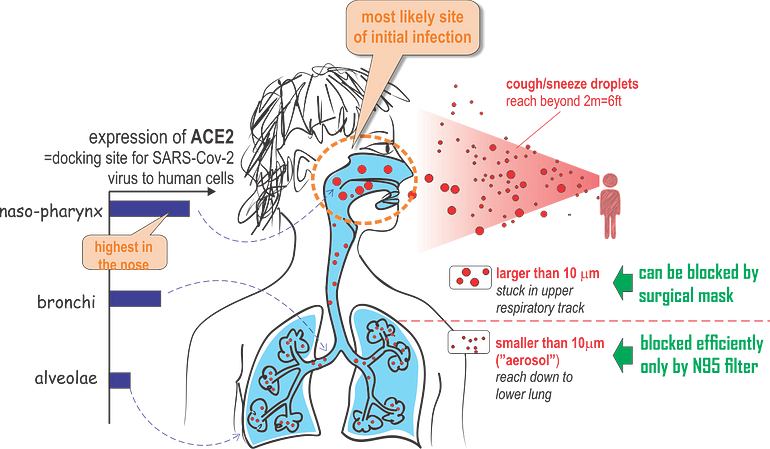
The molecular analysis also show that the SARS-Cov2 virus is active and replicates already in the nasopharynx, unlike other respiratory viruses that dwell in deeper regions of the lung.
-
Surprisingly, ACE2 expression in the lung is very low: it is limited to a few molecules per cell in the alveolar cells (AT2 cells) deep in the lung. But a just published paper by the Human Cell Atlas (HCA) consortium reports that ACE2 is highly expressed in some type of (secretory) cells of the inner nose!
Major route of viral entry is likely via large droplets that land in the nose — where expression of the viral entry receptor, ACE2 is highest. This is the transmission route that could be effectively blocked already by simple masks that provide a physical barrier.
-
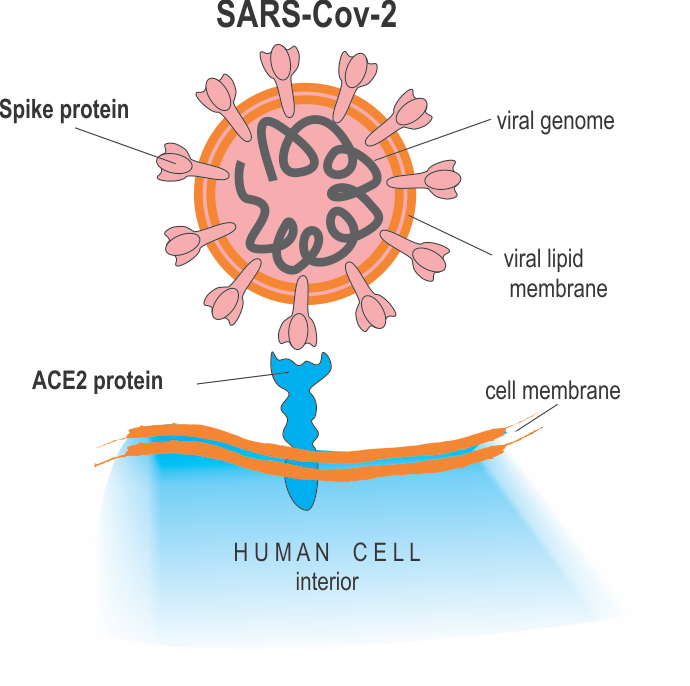
SARS-Cov-2 virus, like any virus, must dock onto human cells using a key-lock principle, in which the virus presents the key and the cell the lock that is complementary to the key to enter the cell and replicate. For the SARS-Cov-2 virus, the viral surface protein “Spike protein S” is the “key” and it must fit snugly into the “lock” protein that is expressed (=molecularly presented) on the surface of the host cells. The cellular lock protein that the SARS-Cov-2 virus uses is the ACE2 protein
SARS-Cov-2 enters the host cell by docking with its Spike protein to the ACE2 (blue) protein in cell surfaces:
-
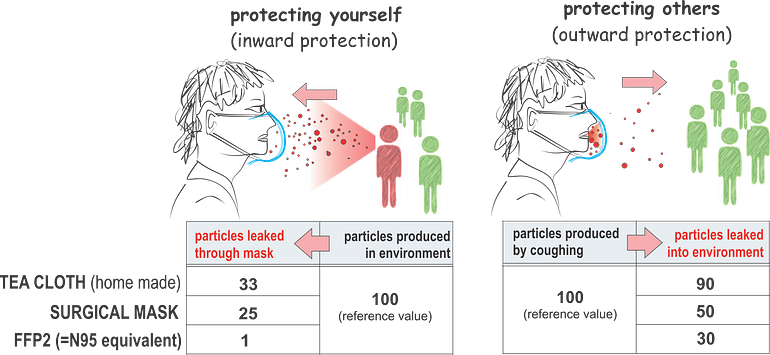
Filtering effect for small droplets (aerosols) by various masks; home-made of tea cloth, surgical mask (3M “Tie-on”) and a FFP2 (N95) respirator mask. The numbers are scaled to the reference of 100 (source of droplets) for illustrative purposes, calculated from the PF (protection factor) values
-
The tacit notion at the CDC that the alveolae are the destination site for droplets to deliver the virus load (the alveolae are after all the anatomical site of life-threatening pneumonia), has elevated the apparent importance of N95 masks and led to the dismissal of surgical masks.
Why N95 masks are much better over the surgical masks
-
In the case of the SARS-Cov-2 virus it is not known what the minimal infectious load is (number of viral particles needed to start the pathogenesis cascade that causes a clinical disease).
Minimal infectious load
-
Of course many aerosol droplets in the exhalation or cough spray may not contain the virus, but some will do.
-
droplets of a typical cough expulsion have a size distribution such that approximately half of the droplet are in the categories of aerosols, albeit they collectively represent only less than 1/100,000 of the expelled volume
Droplets of a typical cough
-
For airborne particles to be inspired and reach deep into the lung, through all the air ducts down to the alveolar cells where gas-exchange takes place, it has to be small
Only droplets < 10 um can reach to alveolae (deep into lung). Larger droplets stuck in the nose, throat, upper air ducts of the lung, trachea and large bronchia.

-
Droplets can (for this discussion) be crudely divided in two large categories based on size
2 categories of droplets:
a) Droplets < 10 um: upper size limit of
aerosol. Can float in the air/rooms by ventilation or winds and can be filtered (to 95%) by N95 favial masks (droplets < than 0.3 um). Here the surgical masks cannot help.b) Droplets > 10 um (reaching 100+ um): called as
spray droplets. Can be even visible by human from coughing/sneezing (0.1+ um).
-
-
www.medrxiv.org www.medrxiv.org
-
doi.org doi.org